
DOP37 Neoplastic lesions outside diseased area in inflammatory bowel disease patients: A national cohort study
A. Cremer1, P. Demetter2, M. De Vos3, J.F. Rahier4, F. Baert5, T. Moreels6, E. Macken6, E. Louis7, S. Vermeire8, D. Franchimont1, Belgian Inflammatory Bowel Disease Research and Development (BIRD) Group
1Department of Gastroenterology, Erasme University Hospital- ULB, Brussels, Belgium, 2Institut Jules Bordet, Department of Pathology, Brussels, Belgium, 3Department of Gastroenterology, University Hospital Ghent, Ghent, Belgium, 4Department of Gastroenterology, CHU UCL Namur, Yvoir, Belgium, 5Department of Gastroenterology, AZ Delta, Roeselare, Belgium, 6Department of Gastroenterology, University Hospital Antwerp, Edegem, Belgium, 7Department of Gastroenterology, University Hospital Liège, Liège, Belgium, 8Department of Gastroenterology, University Hospital Leuven, Leuven, Belgium
Background
Patients with inflammatory bowel diseases (IBD) are at increased risk of dysplasia and colitis-associated cancer (CAC). The presentation of (pre)neoplastic lesions (low-grade dysplasia (LGD), high-grade dysplasia (HGD) or colorectal cancer (CRC) is reported to vary depending if the lesions are located inside disease area (IDA) or outside diseased area (ODA). The primary aim was to analyse the characteristics and prognostic of IDA compared with ODA neoplastic lesions in a large cohort of IBD patients.
Methods
We performed a multicentre retrospective pathological data collection from 7 tertiary referral regional or academic IBD centres in Belgium. Clinical, endoscopic and pathological data were retrieved through retrospective electronic chart review. From the IBD pathology databases, 1183 colorectal lesions were identified in 541 IBD patients: 415 developed dysplasia (77%) and 126 CRC (23%) during their follow-up. Biopsies and surgical specimen were centrally reviewed by an expert IBD pathologist to confirm the diagnosis of dysplasia and/or CRC.
Results
Demographic and clinical variables of the study population are summarised in
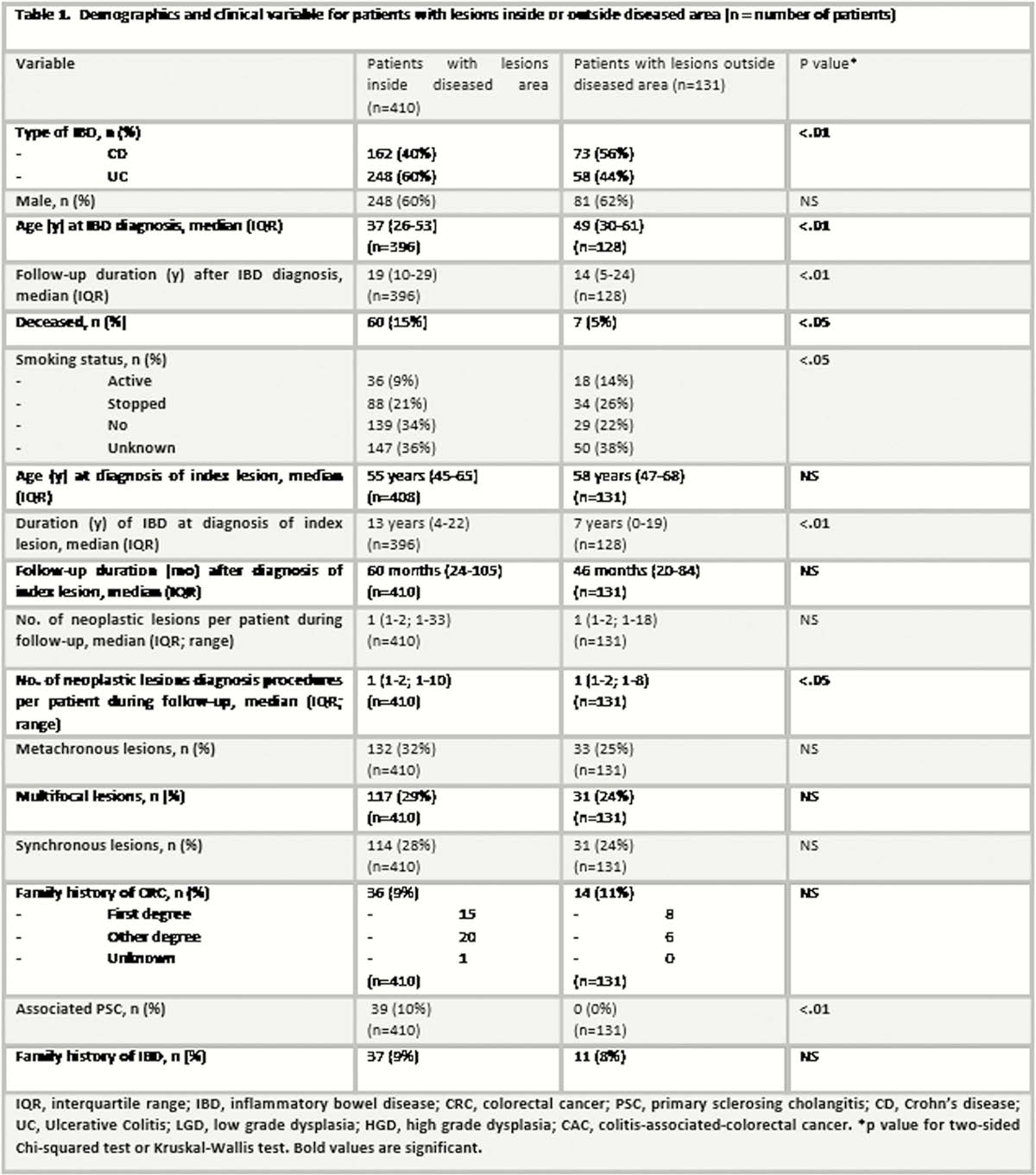
Conclusion
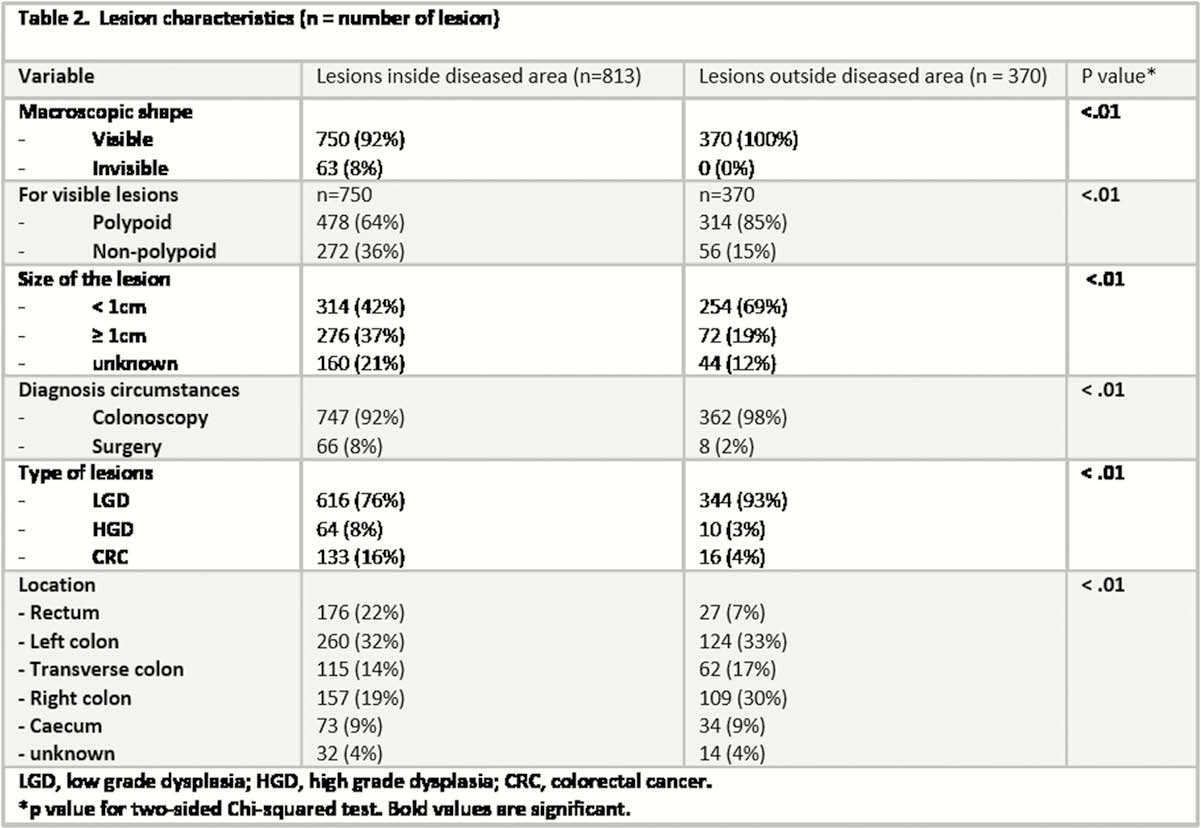
Neoplastic lesions outside the diseased area were more likely to be visible, polypoid, < 1cm, in the right colon and diagnosed at endoscopy than inside disease area lesions. A lower prevalence of HGD and Cancer were reported with neoplastic lesions outside the diseased area.