
DOP38 Prevalence of fatigue in a severe inflammatory bowel disease cohort highly exposed to biologics
C. Liefferinckx1,2, M. El hamdi1, M. Fassin2, A. Cremer1,2, C. Minsart1,2, L. Amininejad1, V. Wambacq1, A. Van Gossum1, D. Franchimont1,2
1Department of Gastroenterology, Hopital Erasme, Brussels, Belgium, 2Laboratory of Experimental Gastroenterology, ULB, Brussels, Belgium
Background
In addition to physical and psychological factors, systemic inflammation, anaemia and/or malnutrition contribute to fatigue in Crohn’s disease (CD) and ulcerative colitis (UC). Despite recent advances in the management of the disease activity, fatigue is a major disabling symptom for inflammatory bowel disease (IBD) patients.
Methods
The aim of this prospective study is to evaluate the prevalence of IBD patients suffering from fatigue in a tertiary IBD referral centre and delineate its contributing factors. All patients with a confirmed IBD diagnosis were eligible. A given written consent has been obtained for each patient (P2019/053). Fatigue evaluation was assessed by FACIT-F. Self-report questionnaires were used to assess different factors related to fatigue: disease activity was assessed by patient-reported outcomes (PRO), anxiety by State and Trait Spielberger scores, depression by Beck score (BDI-II), sleep quality by Insomnia severity index (ISI) and Epworth scale, and quality of life by the Short Inflammatory Bowel Disease Questionnaire (SIBDQ). Biological values including haemoglobin, C-reactive protein (CRP), thyroid-stimulating hormone (TSH), folic acid and B12 vitamin were collected when available.
Results
Demographic data of the 128 included patients are presented in Table 1. This cohort was characterised by a high prevalence of CD complicated behaviours and UC pancolitis. 84.4% of patients (
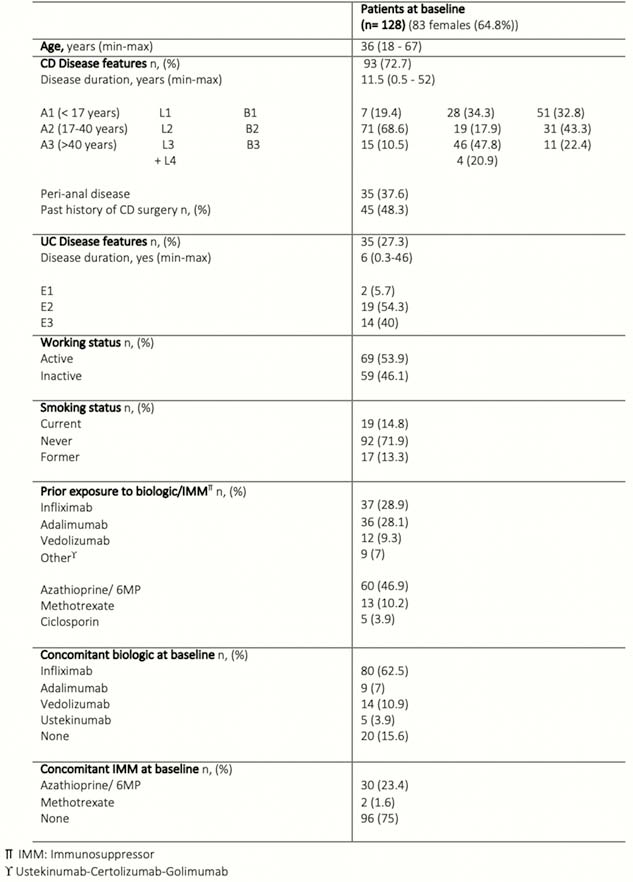
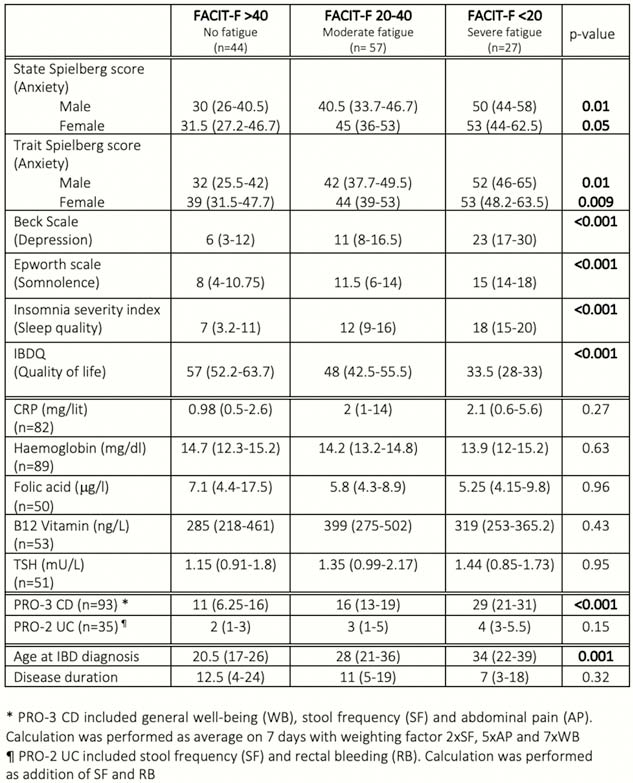
The prevalence of fatigue was 65.6% stratified as severe (FACIT-F <20) and moderate (FACIT-F 20–40) in 21.1% and 44.5%, respectively. Fatigue was clearly associated with active disease in CD, anxiety, depression, poor quality of life, insomnia and somnolence but not with active disease in UC. All biological values were within normal ranges and did not influence fatigue. Older age at diagnosis was associated with lower FACIT-F score while disease duration was not (Table 2). No correlation was found between fatigue and any specific biologics (
Conclusion
This prospective study reported a fatigue prevalence of 65.6% in a severe IBD cohort highly exposed to biologics. Beyond disease activity in CD, psychological factors (whether they are causes or consequences) such as anxiety, depression, poor quality of life and insomnia were associated with fatigue.