
DOP88 Visceral fat area correlates well with anti-TNFα drug levels and secondary loss of response in Crohn’s disease patients
Z. Lim1, C. Welman2, W. Raymond3, L. Thin1,3
1Department of Gastroenterology, Fiona Stanley Hospital, Perth, Australia, 2Department of Radiology, Fiona Stanley Hospital, Perth, Australia, 3School of Medicine and Pharmacology, University of Western Australia, Perth, Australia
Background
A high body mass index (BMI) is known to adversely affect anti-TNFα trough levels and secondary loss of response (SLOR); however, the literature is scarce in defining what aspect of body mass determine these outcomes. We hypothesise that a large visceral fat area is associated with a lower anti-TNFα level and a higher rate of SLOR. Our aim was to determine the impact of fat and muscle compartment areas on these outcomes.
Methods
Crohn’s disease (CD) patients who were prescribed standard doses of an anti-TNFα agent [5 mg/kg, 8 weekly infliximab (IFX) or 40 mg EOW of adalimumab (ADA)] from 1 February 2015 to 30 June 2018 were examined retrospectively. Primary responders with a minimum therapy duration of 12 weeks, at least 12 months of follow-up and a trough level within 6 months of a CT or MRI, were eligible for inclusion. The primary outcome was the trough level and the secondary outcome was time to SLOR, defined as a need to dose escalate, change out of class, requiring ≥3 courses of corticosteroids in a 12-month period, or surgery. Patients were followed until they met a SLOR or the census date of 30 June 2019. Visceral fat area (VFA), subcutaneous fat area (SFA) and skeletal muscle area (SMA) were measured on the CT/MRI at the L3 vertebral level in cm2 by a radiologist blinded to the clinical outcome and corrected for patient height (cm2/m2).
Results
Of 813 patients prescribed an anti-TNFα agent in the study period, data from 69 eligible CD patients were included for analysis. The median age was 43.5 ± 16.2 years, and 42 (60.9%) were males. Forty-four (63.8%) and 25 (36.2%) patients were treated with IFX and ADA respectively. The mean BMI was 26.9 ± 5.2. Univariate analysis of infliximab trough levels found that total fat area, VFA, visceral fat index [VFI (VFA/height in m2)] and VFA/SMA ratio were inversely correlated with anti-TNFα trough level (
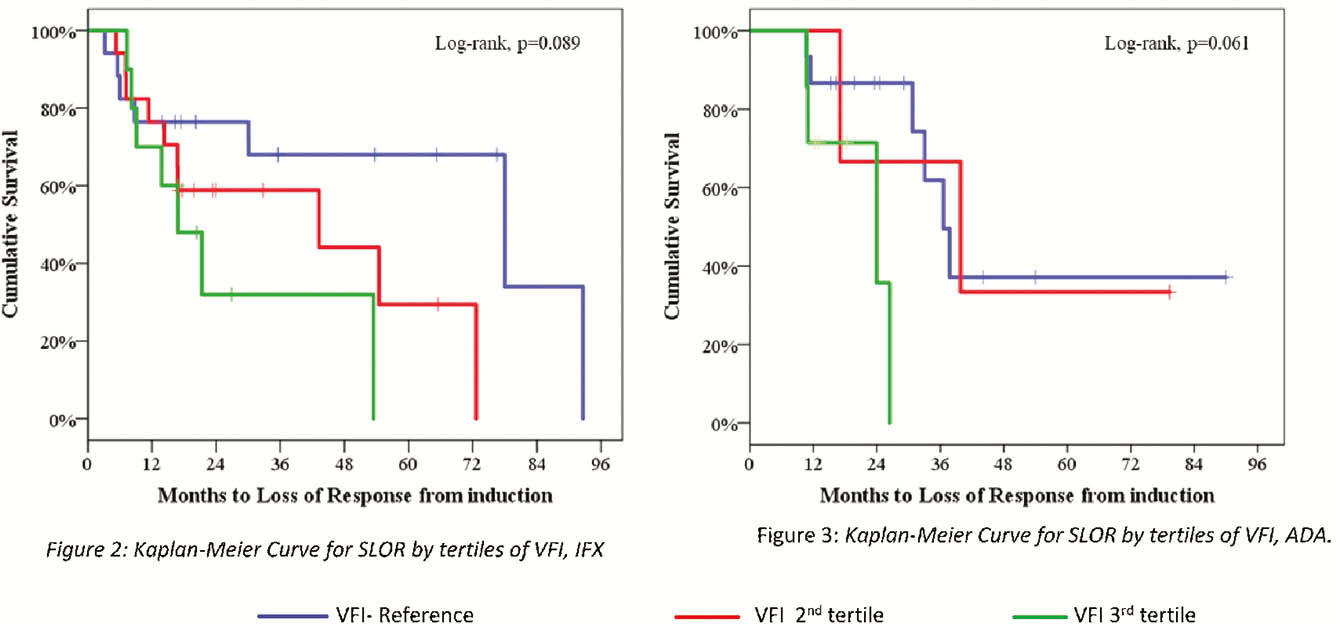
Conclusion
Visceral fat area corrected for height (VFI) is a better determinant of anti-TNFα trough levels and SLOR than BMI.