
DOP90 Physician global assessment of IBD Activity is associated with COVID-19 severity in patients aged less than 50 years
Ricciuto, A.(1);Lamb, C.(2,3);Benchimol, E.I.(1);Walker, G.(4);Kennedy, N.(5,6);Kuenzig, M.E.(1);Kaplan, G.(7);Griffiths, A.M.(1);Reinisch, W.(8);Sebastian, S.(9,10)
(1)The Hospital for Sick Children, Division of Gastroenterology Hepatology and Nutrition, Toronto, Canada;(2)Newcastle University, Gastroenterology, Newcastle upon Tyne, United Kingdom;(3)Newcastle Upon Tyne Hospitals NHS Foundation Trust, Gastroenterology, Newcastle upon Tyne, United Kingdom;(4)Torbay and South Devon NHS Foundation Trust, Gastroenterology, Torbay, United Kingdom;(5)University of Exeter, Gastroenterology, Exeter, United Kingdom;(6)Royal Devon and Exeter NHS Foundation Trust, Gastroenterology, Exeter, United Kingdom;(7)University of Calgary, Gastroenterology, Calgary, Canada;(8)Medical University of Vienna, Gastroenterology, Vienna, Austria;(9)University of Hull, Gastroenterology, Kingston upon Hull, United Kingdom;(10)Hull University Teaching Hospitals NHS Trust, Gastroenterology, Kingston Upon Hull, United Kingdom
Background
SECURE-IBD is an international database that monitors COVID-19 outcomes in IBD patients. We examined the influence of IBD activity (reflected by Physician Global Assessment (PGA)) on COVID-19 severity, while exploring the modifying effect of age.
Methods
We analyzed 3,028 cases reported to SECURE-IBD from March 13-November 17, 2020. PGA was categorized as remission/mild (reference) vs moderate vs severe. Outcomes used as surrogates of severe SARS-CoV2 infection were hospitalization and a composite of ICU/ventilation/death. Using generalized estimating equations (GEE) to account for clustering by country, we determined the unadjusted association between disease activity and COVID-19 outcomes, overall and by age decade. We included the following covariates in multivariable GEE models a priori: time of COVID-19 diagnosis, age, sex, comorbidities (0, 1, ≥2), IBD type, systemic corticosteroids (CS), anti-TNF monotherapy, anti-TNF plus immune modulator, immune modulator monotherapy, and mesalamine. We included additional covariates (country GDP, race, BMI, anti-integrins and ustekinumab) if they changed the estimate by ≥10%. We also built models stratified by age; the age cut-off for stratification was determined using Joinpoint regression (selecting the age at which outcome rates significantly changed).
Results
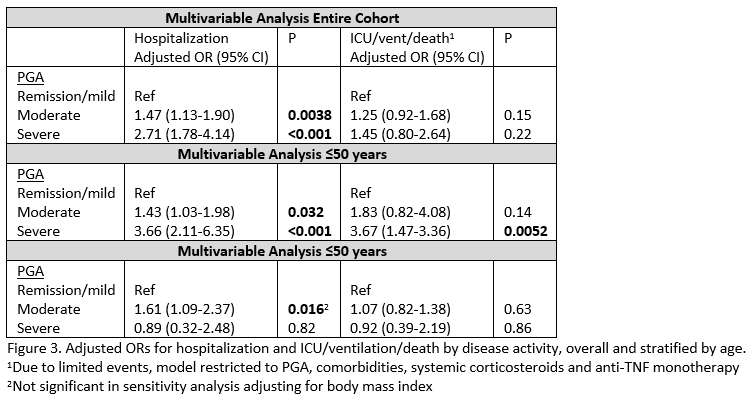
COVID-19 was more severe in patients with more active IBD: hospitalization rates 19% (remission/mild), 26% (moderate) and 45% (severe); ICU/ventilation/death rates 5% (remission/mild), 6% (moderate) and 12% (severe) (p<0.05, Figure 1). In unadjusted analyses, higher PGA was associated with an increased risk of hospitalization (moderate: OR 1.53, 95% CI 1.24-1.88; severe: OR 3.30, 95% CI 2.44-4.46) and ICU/ventilation/death (moderate: OR 1.44, 95% CI 1.10-1.87; severe: OR 2.58, 95% CI 1.71-3.90). As per Figure 2, the magnitude of association between severe PGA (vs remission/mild) and adverse outcomes was greatest in patients ≤50 years. Joinpoint regression also supported a significant change in the rate of ICU/ventilation/death at 50 years. In multivariable analyses (Figure 3), PGA remained significantly associated with hospitalization, but not ICU/ventilation/death. However, in multivariable analyses stratified by age, PGA was consistently associated with both hospitalization and ICU/ventilation/death in patients ≤50, but not >50 years.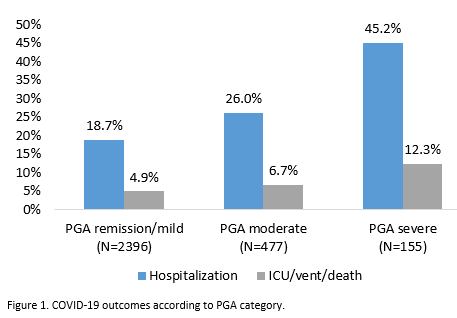

Conclusion
Our data suggest an association between IBD activity, as assessed by PGA, and severe COVID-19 outcome with an increased risk in younger patients. Adequate IBD treatment despite the pandemic is needed to avert poor outcome to symptomatic SARS-CoV2 infections.