
P026 The impact of different dietary factors in the etiopathogenesis of inflammatory bowel disease: a retrospective case–control study
C.M. Preda1, T. Manuc1, A.E. Chifulescu1, D. Istratescu1, E. Louis2, M. Diculescu1, T. Cristian3, L.S. Gheorghe1, M. Manuc1
1Department of Gastroenterology, Department of Digestive Diseases and Liver Transplantation, Clinical Institute Fundeni, Bucharest, Romania, 2Department of Gastroenterology, University Hospital CHU Liège, Liège, Belgium, 3Department of Gastroenterology and Hepatology, Elias Emergency Hospital, Bucharest, Romania
Background
Inflammatory bowel disease development has been associated with several environmental factors, among which diet can play a key role, probably due to a westernised lifestyle. However, its involvement in the pathogenesis of IBD is difficult to be demonstrated. The aim of this study was to analyse dietary composition in a Romanian and Belgian population with IBD.
Methods
We conducted an observational retrospective comparative study using two European cohorts (Romanian and Belgian). The IBD group included 76 Romanian and 53 Belgian patients with an IBD diagnosis while the control group included 56 healthy persons (35 Romanians and 21 Belgians). All subjects were interviewed and asked to fill in a questionnaire regarding diet.
Results
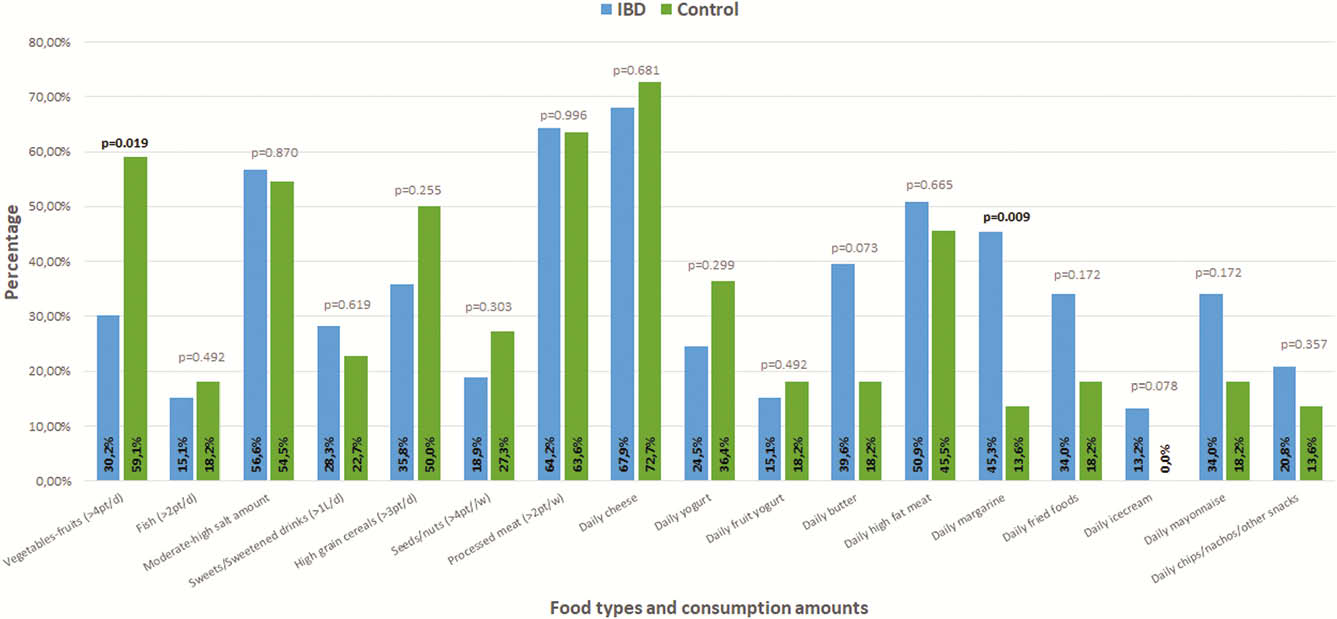
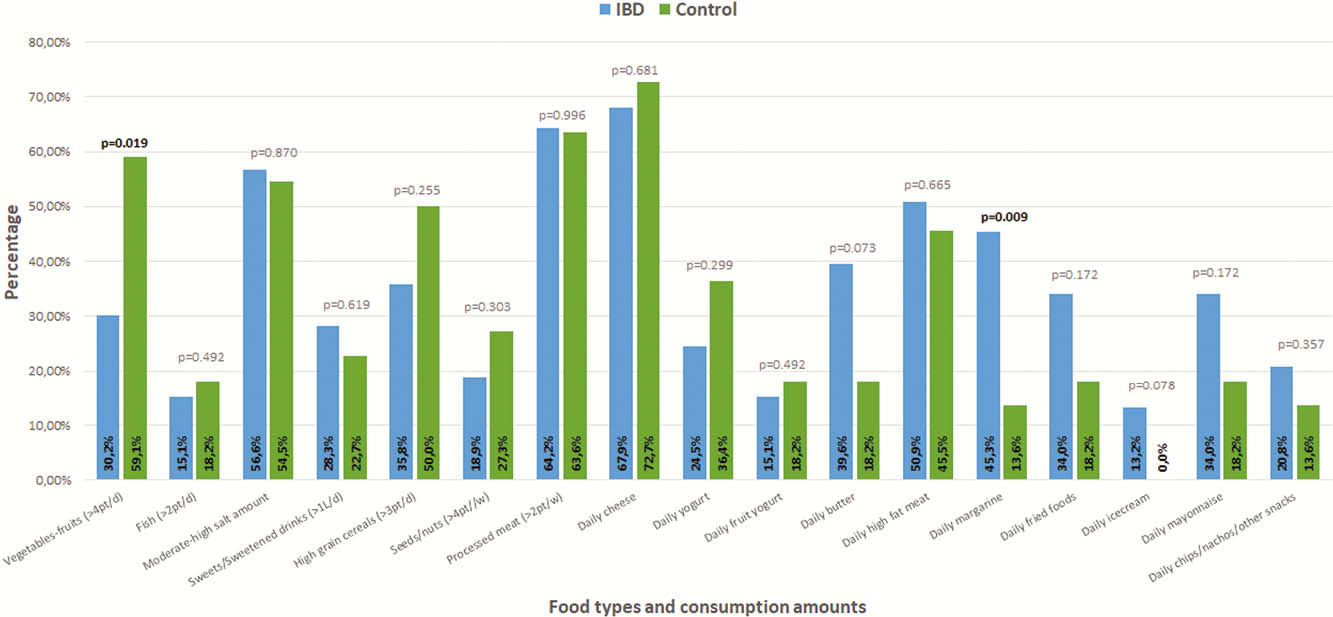
The baseline characteristics of the patients included in the two cohorts were described in the table. Figures 1 and 2 illustrated the consumption of different foods in Romanian, respectively, Belgian IBD patients before the onset of the disease vs. healthy controls (variables were compared with Fisher’s exact test). In the entire IBD cohort (Romanian+Belgian), we found a significantly increased consumption of sweets (OR 3.36[95% CI 1.6,7]), processed and high-fat meat (OR 2.5[95% CI1.4, 4.7], fried food (OR 9.5[3.8, 23.6]), salt (OR 2.8[1.5, 5.3]), ice cream (OR 3.25[1.1, 9.8]), mayonnaise (OR 3.49[1.1, 10.3]), margarine (OR 5.63[1.64, 19.33]), chips/nachos/other snacks (OR 2.3[0.97, 5.73]), compared with the healthy control group. The intake of seeds, nuts (OR 0.26[0.14,0.52]) and the yoghurt consumption (OR 0.44[0.23, 0.83]) was lower in the IBD group compared with the control group.
| Variable | Romanian CD patients ( | Belgian CD patients ( | |
| Males (%) | 43.5% | 32.6% | 0.383 |
| Median age (min ÷ max) | 42 years (19 ÷ 67 years) | 42 years (19 ÷ 73 years) | 0.183 |
| Median disease duration | 3 years (0.5 ÷ 14 years) | 10 years (1 ÷ 42 years) | <0.001 |
| A1/A2/A3 | 0/73.9/26.1% | 15/75/10% | 0.005 |
| L1/L2/L3 | 26.1/34.8/39.1% | 30/12.5/57.5% | 0.335 |
| B1/B2/B3 | 45.4/27.3/27.3% | 60/20/20% | 0.208 |
| Upper GI tract location (L4) | 4.3% | 11.4% | 0.231 |
| Perianal disease | 13% | 40% | 0.006 |
| Variable | Romanian UC patients ( | Belgian UC patients ( | |
| Males (%) | 66.7% | 20% | 0.025 |
| Median age (min ÷ max) | 41 years (28 ÷ 74 years) | 43.5 years (26 ÷ 64 years) | 0.569 |
| Median disease duration | 6 years (0.5 ÷ 15 years) | 11.5 years (1 ÷ 16 years) | 0.158 |
| E1/E2/E3 | 6.7/53.3/40% | 0/77.8/22.2% | 0.588 |
Conclusion
In Romanian and Belgian IBD patients, a westernised diet with increased consumption of sweets, processed food, high-fat meat, fried food, salt, margarine, snacks, ice cream and mayonnaise seems to be a risk factor for IBD. Food intake of seeds, nuts and yogurt may be a protective factor.