
P159 Histopathological findings of preclinical inflammatory bowel disease
I. Rodríguez-Lago1, O. Merino2, I. Azagra3, A. Maiz4, E. Zapata5, R. Higuera6, I. Montalvo7, M. Fernández-Calderón8, P. Arreba9, J. Carrascosa10, A. Iriarte11, M. Muñoz-Navas12, J.L. Cabriada1, M. Barreiro-de Acosta13
1Hospital de Galdakao, Gastroenterology, Bilbao, Spain, 2Hospital Universitario de Cruces, Gastroenterology, Barakaldo, Spain, 3Hospital Universitario Araba, Gastroenterology, Vitoria, Spain, 4Hospital Universitario Donostia, Gastroenterology, Donostia, Spain, 5Hospital de Mendaro, Gastroenterology, Mendaro, Spain, 6Hospital de San Eloy, Gastroenterology, Barakaldo, Spain, 7Onkologikoa, Gastroenterology, Donostia, Spain, 8Hospital de Mondragón-Alto Deba, Gastroenterology, Mondragón, Spain, 9Hospital Universitario de Basurto, Gastroenterology, Bilbao, Spain, 10Hospital de Zumárraga, Gastroenterology, Zumárraga, Spain, 11Hospital Bidasoa, Gastroenterology, Irún, Spain, 12Clínica Universidad de Navarra, Gastroenterology, Pamplona, Spain, 13Hospital Clínico Universitario de Santiago de Compostela, Gastroenterology, Santiago de Compostela, Spain
Background
The diagnosis of inflammatory bowel disease (IBD) is usually established after the development of symptoms, but preclinical disease may be present years before the final diagnosis. Recently, histology has become one of the main outcomes of IBD treatment. The primary aim of our study was to define the main histological findings of preclinical IBD and its association with the natural history of the disease.
Methods
This multicentric, retrospective study included all patients who participated in the colorectal cancer screening programme in 11 centres between 2009–2014. All patients were firstly assessed by a faecal immunochemical test (OC-Sensor, Eiken Chemical Co., Tokyo, Japan) and, if this test was positive (cut-off 20 μg Hgb/g), a colonoscopy was performed. All patients had an incidental diagnosis of IBD confirmed by histology, according to current ECCO criteria, during a screening colonoscopy. Three histologic findings were evaluated at diagnosis: presence of granuloma, crypt abscesses and/or eosinophilic infiltrate. The main outcomes were the development of symptoms and the risk of proximal disease extension. The frequency of each finding was described separately by IBD subtype and the chi-square test was used to describe possible association with the main outcomes.
Results
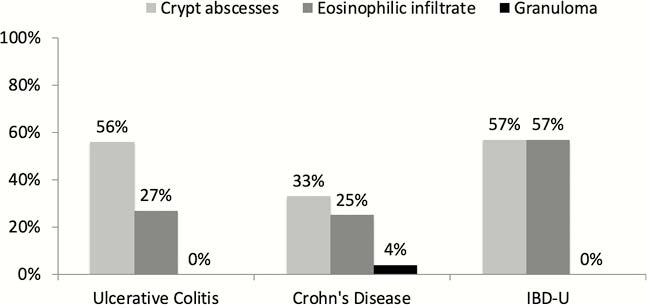
During this period we performed 31,005 colonoscopies after 498,227 FIT. Finally, 110 patients were included with an incidental diagnosis of ulcerative colitis (UC, 79 cases), Crohn’s disease (CD, 24 cases) or IBD-Unclassified (IBD-U, 7 cases). Crypt abscesses were present in 56%, 33% and 57% of UC, CD and IBD-U patients, respectively (Figure 1). An eosinophilic infiltrate was observed in 27%, 25% and 57% of patients, respectively. Granuloma were only observed in 4% of CD patients. There were no statistically significant differences in these findings according to IBD subtype (
Conclusion
Preclinical IBD is frequently associated with the presence of crypt abscesses, especially in UC. Granuloma is probably a late finding in CD. Around one third of patients show a eosinophilic infiltrate in the early phases of the disease.