
P202 De novo Inflamatory Bowel Disease after solid organ transplantation
Luque Carmona, A.M.(1);Rojas Feria, M.(1);De la Cruz Ramirez, M.D.(1);Trigo Salado, C.(1);Herrera Justiniano, J.M.(1);Leo Carnerero, E.(1);
(1)Hospital Universitario Virgen del Rocío, Digestive Diseases Unit, Sevilla, Spain
Background
The aim of this study was to determine the disease phenotype, evolution and therapeutic needs of de novo inflammatory bowel disease (IBD) in transplanted patients.
Methods
A retrospective single center study that included all patients who developed IBD after solid organ transplantation in a tertiary hospital. Data collected included transplant-related variables, IBD phenotype, course of the disease and its treatment. A control group of non-transplanted IBD patients was randomly selected.
Results
We included 17 post-transplanted IBD patients and 57 non-transplanted IBD patients. Post-trasplanted patients were older at diagnosis, had greater colonic involvement, with an inflammatory behaviour, absence of perianal involvement and extraintestinal manifestations compared to control group (Table 1).
The most common immunosuppression regimen was tacrolimus+mycophenolate mofetil (MMF)+prednisone and the most frequent change after diagnosis was the switch of MMF for azathioprine. De novo IBD patients required less biological therapy than the control group (11.8 vs 42.1% p 0.02) and none required surgical intervention compared to 35.1% in the control group (p 0.002).
Multivariate analysis carried out on the total population showed that active smoking, perianal disease and extraintestinal manifestations were associated with a greater need for biologics, while the only factor that influenced surgical risk was stricturing and penetrating behaviour of Crohn´s disease.
Figure 1. Total transplants performed in our hospital and patients who developed de novo IBD after transplantation.
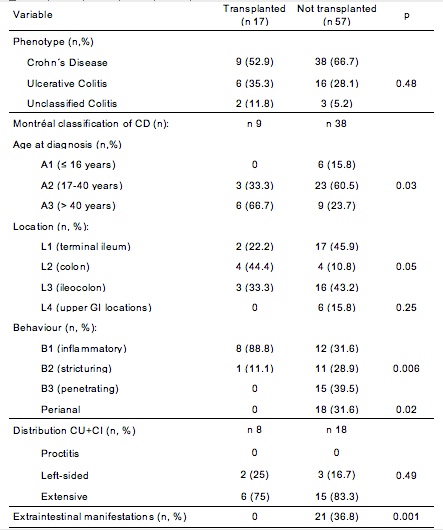
Table 1. Phenotypic characteristics.
Conclusion
De novo IBD after solid organ transplantation has a favorable course, predominating the inflammatory behaviour and requiring less biological therapy and surgical interventions. The absence of extraintestinal manifestations and perianal disease stands out.