
P203 The performance of the Rutgeerts’ score, SES-CD, and MM-SES-CD for prediction of post-operative clinical recurrence in Crohn’s disease
Narula, N.(1);Wong, E.(1);Dulai, P.(2);Marshall, J.(1);Jairath, V.(3);Reinisch, W.(4);
(1)McMaster University, Department of Medicine Division of Gastroenterology, Hamilton, Canada;(2)University of California San Diego, Division of Gastroenterology, La Jolla, United States;(3)Western University, Department of Medicine Division of Gastroenterology, London, Canada;(4)Medical University of Vienna, Department of Internal Medicine III Division of Gastroenterology and Hepatology, Vienna, Austria;
Background
Prevention of post-operative recurrence in Crohn’s disease (CD) is important to avoid further complications requiring additional surgeries. The Rutgeerts’s score is currently the gold standard assessment in clinical trials of post-operative CD. However, the Simplified Endoscopic Score for CD (SES-CD) has not been validated or used clinically in post-operative CD patients. The Modified Multiplier of the SES-CD (MM-SES-CD) is a novel internally validated tool that was developed to account for differences in items of the SES-CD and has not yet been validated in the setting of post-operative CD. The purpose of this study was to compare the SES-CD and MM-SES-CD scores with the Rutgeerts’ score for predicting clinical recurrence (CR) of post-operative CD.
Methods
This was a post-hoc analysis of data from the phase 3 PREVENT trial (ClinicalTrials.gov identifier: NCT01190839) of 208 participants who received infliximab or placebo. Receiver operating characteristic curve analyses to compare the Rutgeerts’, ileum SES-CD, and ileum MM-SES-CD scores at week 76 with CR at week 104. Multivariate logistic regression models evaluated cut-offs for the odds of achieving week 104 CR, after adjustment for confounders, including treatment allocation, disease duration, prior anti-TNF use, and concomitant immunomodulator use. CR was defined as CDAI score ≥200 and ≥70 point increase from baseline (or development of fistulas, abscesses, or treatment failure) and endoscopic recurrence, defined as Rutgeerts’ score ≥i2.
Results
The Rutgeerts’ score predicted week 104 CR at with fair accuracy [AUC: 0.74 (95% CI: 0.65-0.83)], which was similar to the SES-CD ileum score [AUC: 0.72 (95% CI: 0.64-0.80)] and the MM-SES-CD ileum score [AUC: 0.72 (95% CI: 0.63-0.80)]. Compared to various cut-offs by the other scores, the MM-SES-CD ileum score ≥26 at week 76 had the best ability to predict week 104 CR. Patients with a week 76 MM-SES-CD ileum score ≥26 were 4.17 times (95% CI: 1.90-9.12, p <0.001) more likely to have CR compared to those with a MM-SES-CD ileum score <26.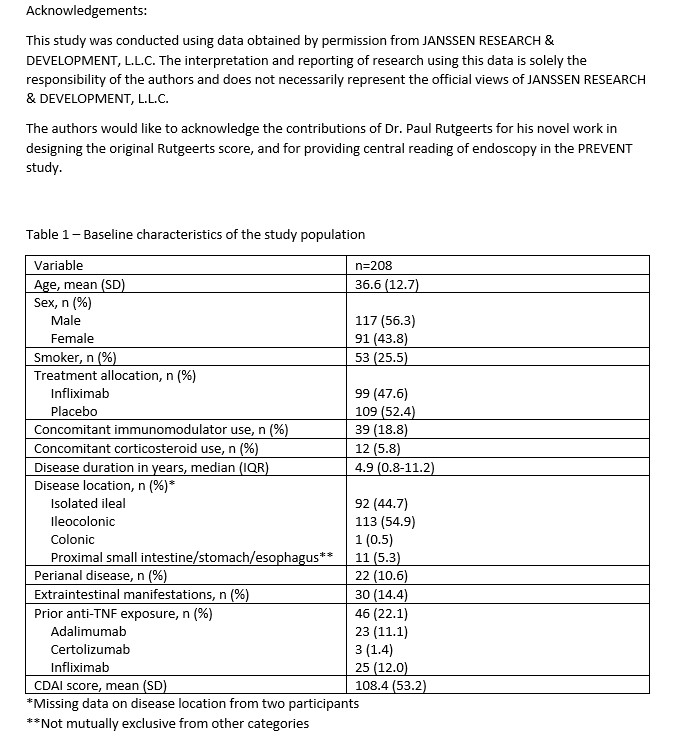


Conclusion
The ileal SES-CD and ileal MM-SES-CD perform similarly to the Rutgeerts’ score for predicting CR of post-operative CD. The MM-SES-CD threshold of ≥26 best predicted post-operative CR. Clinicians and trialists should consider the use of the MM-SES-CD in the assessment of post-operative CD given its performance and ability to capture colonic disease recurrence.