
P252 Solid organ transplant (with the exception of liver) in patients with inflammatory bowel disease: An ECCO CONFER Multicentre Case Series
Ribaldone, D.G.(1)*;Vieujean, S.(2);Julsgaard, M.(3);Zingone, F.(4);Savarino, E.(4);Cañete, F.(5);Aratari, A.(6);Imperatore, N.(7);Ramos, L.(8);Plaza, R.(9);Pugliese, D.(10);Barberio, B.(4);Drobne, D.(11);Chaparro, M.(12);
(1)University of Turin, Department of Mediical Sciences, Turin, Italy;(2)University Hospital CHU of Liège, Hepato-Gastroenterology and Digestive Oncology, Liège, Belgium;(3)Aarhus University Hospital, Department of Hepatology and Gastroenterology, Aarhus, Denmark;(4)University of Padova, Division of Gastroenterology- Department of Surgery Oncology and Gastroenterology DiSCOG, Padova, Italy;(5)Hospital Universitari Germans Trias i Pujol., IBD Unit. Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas CIBEREHD., Badalona. Madrid., Spain;(6)San Filippo Neri Hospital, IBD Unit, Roma, Italy;(7)AORN Antonio Cardarelli of Naples, Gastroenterology and Endoscopy Unit, Napoli, Italy;(8)Hospital Universitario de Canarias- Universidad de La Laguna, Gastroenterology and Hepatology Department, Tenerife, Spain;(9)Hospital Universitario Infanta Leonor, Gastroenterology Department, Madrid, Spain;(10)Fondazione Policlinico Universitario 'A. Gemelli' IRCCS, CEMAD- IBD CENTER- Unità Operativa Complessa di Medicina Interna e Gastroenterologia- Dipartimento di Scienze Mediche e Chirurgiche, Roma, Italy;(11)University Medical Centre Ljubljana, Department of Gastroenterology, Ljubljana, Slovenia;(12)Hospital Universitario de La Princesa, Servicio de Aparato Digestivo, Madrid, Spain;
Background
There are limited data available on the course of IBD in patients with solid organ transplantation.
The aim of this ECCO CONFER study was to evaluate the trend of IBD before and after solid organ transplantation but liver.
Methods
This was a retrospective observational multicentre study that collected cases through the CONFER project. Patients with an established IBD diagnosis who underwent a solid organ transplantation (with the exception of liver) were eligible candidates.
Results
33 patients with solid organ transplantation (67% male; 55% CD) were collected from 12 referral centres in five different countries.
Mean age was 53 ± 16 years. 34 organs were transplanted in 33 patients. Most of the patients underwent kidney transplantation (n=27, 82%). 4 (12%) received a heart and 1 (3%) underwent lung transplantation; 1 (3%) underwent a combined heart and kidney transplant.
The mean duration of IBD was 18.4 ± 14.7 months. Clinical characteristics are summarized in Table 1.
The median follow-up after transplantation was 4.3 years (IQR 3.25 – 10.7).
7/33 patients (21.2%) experienced organ rejection, with 1 kidney retransplant.
Regarding immunosuppressive therapy, 29/33 patients (88%) were treated with tacrolimus, 25 (76%) with systemic steroids, 22 (67%) with mycophenolate mofetil, 11 (33%) with everolimus, 6 with cyclosporine (18%), 3 (9%) with thiopurines. Regarding biologics, 1 patient was treated with infliximab, 2 with adalimumab, 2 with vedolizumab, 1 with ustekinumab.
Defining a severe IBD course the need for biologic therapy or bowel resection or hospitalization, 4 patients (11.7%) had a severe disease course after transplantation versus 3 patients (9.3%) in the first 51 months of disease before transplantation (p = 0.26). Univariate analysis is reported in Table 2.
1 case of low-grade dysplasia was found 10 years after the transplantation. 1 case of colorectal cancer was found in a patient affected by CD five years after kidney transplantation. The other cases of tumours after transplantation are reported in Table 3.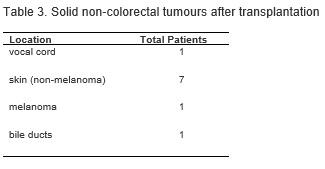
The first serious infectious episode after transplantation is shown in Table 4: 17 of 33 patients (51.5%) reported at least 1 episode of serious infection. 
In total 29 different serious infectious episodes after transplantation were recorded, compared to 28 episodes in the pre-transplantation period.
At the last follow-up visit, 6/33 (18.2%) patients had died: 1 due to cholangiocarcinoma, 1 amyloidosis, 1 heart failure, 1 myocardial infection (2 not available).
Conclusion
Solid organ transplantation appears to have a satisfactory course for both the transplanted organ and IBD, in terms of organ survival and IBD severity; furthermore, the use of biologics in these patients does not appear to be linked to a worse outcome.