
P307 Colorectal neoplasia risk in patients with inflammatory bowel disease and serrated lesions
M. De Jong1, S. Vos2, I. Nagtegaal2, Y. van Herwaarden1, L. Derikx1, F. Hoentjen1
1Department of Gastroenterology and Hepatology, Radboud University Medical Center, Nijmegen, The Netherlands, 2Department of Pathology, Radboud University Medical Center, Nijmegen, The Netherlands
Background
The presence of serrated lesions (SLs) is an established risk factor for colorectal neoplasia development in the general population. However, the impact of SLs on the colorectal neoplasia risk in inflammatory bowel disease (IBD) patients is unknown. In addition, SLs might have been misclassified in IBD patients in the past, in part due to revisions of classification systems. Presently, SLs are categorised as hyperplastic lesions, sessile SLs, and traditional serrated adenomas. We aimed (1) to compare the colorectal neoplasia risk in IBD patients with SLs vs. IBD patients without SLs, and 2) to study the subclassification of SLs in IBD patients before and after histopathological review by two expert gastrointestinal pathologists.
Methods
We identified all IBD patients with colonic SLs from 1996 to 2019 in a tertiary referral centre using the local histopathology database. Patients with neoplasia prior to SL diagnosis were excluded. Clinical data from patients’ charts were retrieved until June 2019. A subgroup of 135 SLs was reviewed by two pathologists. The log-rank analysis was used to compare the cumulative (advanced) neoplasia incidence in IBD patients with SL vs. IBD patients without SL undergoing surveillance in the same time period. Patients were censored at the end of surveillance or at colectomy.
Results
We identified 376 SLs in 204 IBD patients (61.9% ulcerative colitis (UC)). In the original reports, 91.9% was classified as a hyperplastic lesion. After histopathological review, 120/136 (88%) of the SLs were confirmed (16 were no SL). Of the 120 confirmed SLs, 62.2% was classified as a sessile SL, 37.8% as a hyperplastic lesion, and 0.8% as a traditional serrated adenoma. The mean time from IBD diagnosis to the first serrated lesion was 14.3 ( ± 12.3) years. A total of 41/204 (20.0%) of patients developed neoplasia (3 CRC, 3 HGD, and 35 LGD; including 2 HGD and 17 LGD at the moment of serrated lesion detection). In the 304 patients without SL (52.6% UC), 63 developed neoplasia (20.7%; 8 CRC, 5 HGD and 50 LGD). Patients who received follow-up colonoscopies after SL (
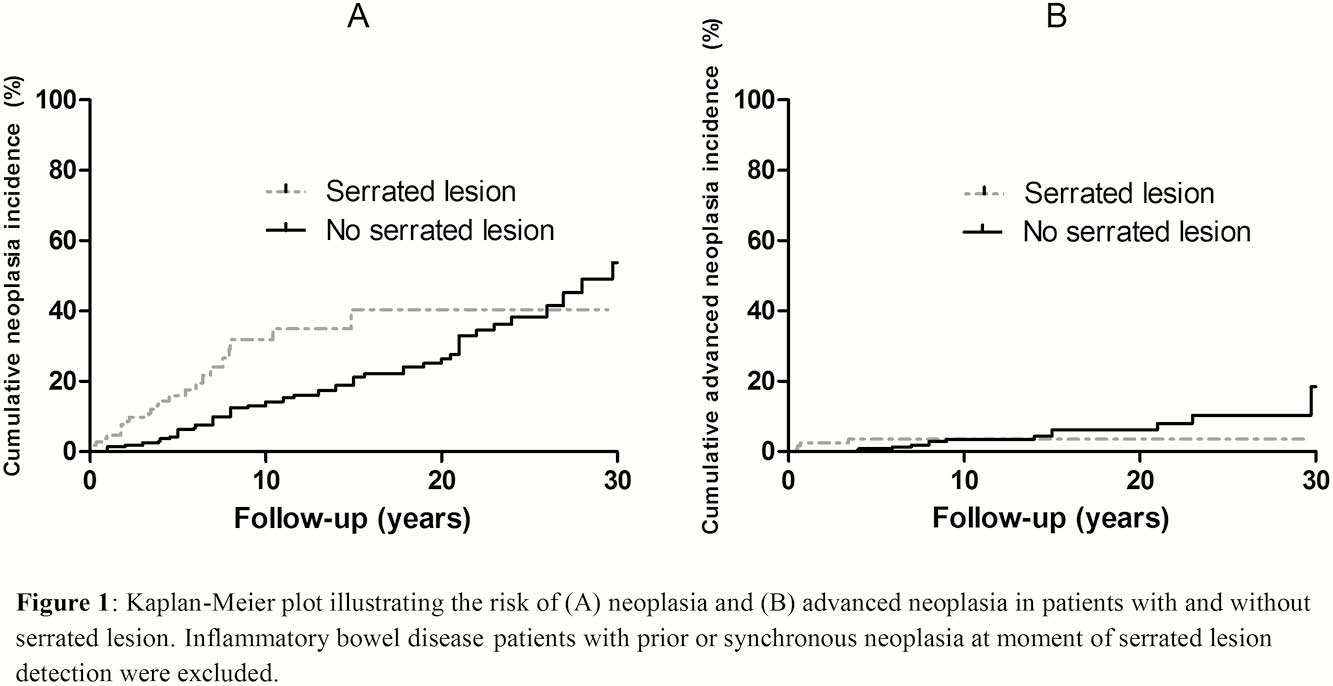
Conclusion
The presence of SLs in IBD patients was associated with a relatively high risk of synchronous colorectal neoplasia as well as an increased risk of subsequent neoplasia, although not with an increased risk of advanced neoplasia. Histopathological review confirmed the SL diagnosis in the majority of lesions, although a large proportion of the hyperplastic lesions was reclassified as a sessile SL.