
P520 Very early intestinal ultrasound predicts intravenous corticosteroid failure in hospitalized severe ulcerative colitis patients
Fremberg Ilvemark, J.(1);Wilkens, R.(2);Thielsen, P.(1);Kirch Dige, A.(3);Boysen, T.(2);Brynskov, J.(1);Tveiten Bjerrum, J.(1);Seidelin, J.(1);
(1)Herlev University Hospital, Department of Gastroenterology and Hepatology, Copenhagen, Denmark;(2)Hvidovre University Hospital, Gastrounit- Medical Division, Copenhagen, Denmark;(3)Aarhus University Hospital, Department of Gastroenterology and Hepatology, Aarhus, Denmark;
Background
Intestinal ultrasound (IUS) is an objective marker for inflammation in ulcerative colitis (UC). Few studies have examined if repeated IUS can predict treatment outcomes in UC. Our aim was to determine if IUS changes after 48±24h of intravenous corticosteroids can predict treatment outcomes in hospitalized patients with severe UC.
Methods
We performed a blinded observational multicenter study at three university hospitals in Denmark. Bowel wall thickness (BWT), colour doppler signals (CDS), inflammatory mesenteric fat (I-fat), haustration, and bowel wall stratification (BWS) were assessed before treatment initiation and after 48±24h. Treatment response was assessed with a partial Mayo score (pMayo) at day 6±1, defined as a ≥30% and ≥3 point reduction with either a rectal bleeding subscore of 0 or 1 OR a decrease in rectal subscore ≥1 point. If infliximab was administered earlier (≥3 days), pMayo was evaluated at administration. The treating physician was blinded to the IUS findings, and the IUS examiner was blinded to all non-IUS disease parameters.
Results
Fifty-six patients were recruited between February 2019 and March 2021 (Table 1). Thirty-seven (66%) responded to intravenous corticosteroid therapy within seven days of treatment, while 19 (34%) did not. There was no difference in baseline BWT between groups. However, at follow-up, significant differences between responders and non-responders were identified in both absolute BWT (median 3.1mm vs 4.9mm), absolute reduction ΔBWT (median -1.9mm vs -0.2mm), and percentage reduction (median -35.9% vs -4.1%) all p<0.005, (Figure 1). Receiver operating characteristic curve analysis for BWT at 48±24h to predict non-response showed an area under the curve of 0.85. BWT ≥4mm had a sensitivity of 84.2 (95% CI 60.4-96.6), specificity of 75.7 (95% CI 58.8-88.2), a negative predictive value of 90.3 (95% CI 74.2–98.0), and a positive predictive value of 64 (95% CI 42.5–82.0) for determining non-response. The absence of I-fat, and the presence of BWS and haustration all had significant odds ratio (OR) for detecting response at follow-up. However, BWT was the only significant parameter in the multivariable analysis and, thereby, the most important parameter for response assessment (BWT >20% reduction adjusted OR 10.8 (95% CI 2.5 - 56.6) and BWT ≤4mm adjusted OR 8.8 (95% CI 1.9 - 51.3), both p<0.01). 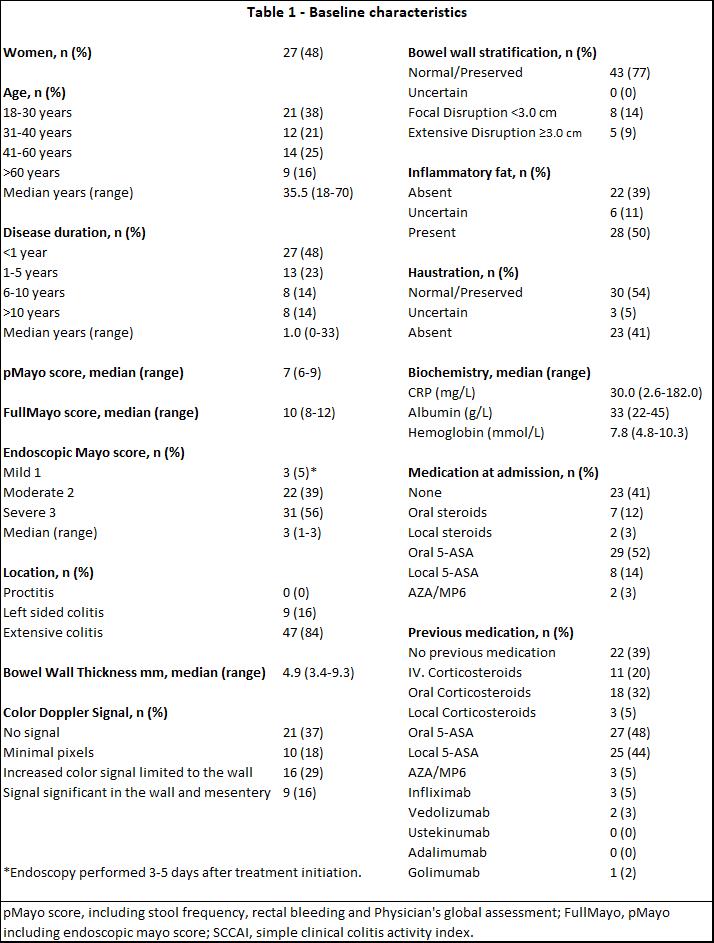

Conclusion
Changes in IUS BWT after 48±24h following intravenous corticosteroid treatment in hospitalized severe ulcerative colitis patients, identify responders with high accuracy. IUS might be utilized as an early corticosteroid non-response marker to guide accelerated rescue infliximab regimes.