
P536 Early prediction of intravenous corticosteroid therapy failure in moderate–severe ulcerative colitis
A. Croft1, A. Lord2, G. Radford-Smith1
1Department of Gastroenterology and Hepatology, Royal Brisbane and Women’s Hospital, Brisbane, Australia, 2QIMR-Berghofer Medical Research Institute, Gut Health Group, Brisbane, Australia
Background
An episode of acute severe ulcerative colitis (UC) is a watershed event during the disease course with a heightened risk of colectomy during and following these episodes.1 The prompt identification of these events followed by the early implementation of appropriate treatment is essential to obtaining the best clinical outcomes for these unwell patients. The majority of published risk scores predicting the important clinical outcomes of intravenous corticosteroid therapy failure and colectomy-by-discharge rely on clinical data from days 1–3 of therapy.2 There is a paucity of tools that allow for a simple and individualised prediction of risk of corticosteroid therapy failure during the earliest stages of admission.
Methods
Data were prospectively obtained from 349 presentations of moderate–severe UC requiring hospital admission to a tertiary referral hospital. The failure of intravenous corticosteroid therapy was strictly defined by the (Oxford) Day 3 and Day 7 criteria.3 Seventeen clinical, laboratory and endoscopic variables all available within 24 h of hospital presentation were assessed for their ability to differentiate intravenous corticosteroid therapy responders from non-responders. A stepwise generalised linear model was formulated based on the results of the initial univariate analyses.
Results
Intravenous corticosteroid therapy failure occurred in 208/349 (60%) of presentations. The formulated risk score included the variables of oral corticosteroid therapy failure, bowel frequency and serum albumin concentration with or without the Mayo endoscopic subscore (MES). With the addition of the MES, the area under the curve (AUC) of the risk score was 0.758. When the positive predictive value of the score (threshold) for correctly predicting intravenous corticosteroid therapy failure was set at 85%, 105/275 (38%) of presentations with available data were identified as high risk for corticosteroid therapy failure (Figure 1).
PPV for corticosteroid failure and success at various thresholds of corticosteroid failure risk score results (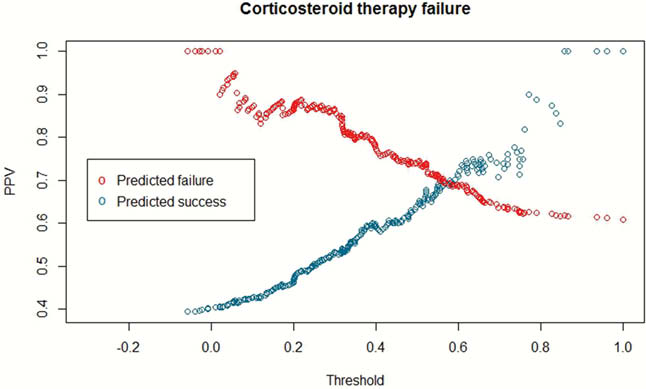
Conclusion
This practical risk assessment tool provides clinicians with a personalised prediction of the likelihood of success of a course of intravenous corticosteroid therapy in moderate–severe UC. It enables the identification of individuals at high risk of treatment failure who may be suitable for consideration of early treatment escalation or screening for appropriate clinical trials.
Williams JG,
Turner D,
Travis SPL,