
P541 Are we addressing the top ten research priorities in IBD?
J. Geldof1, J.F. LeBlanc1, L. Lucaciu2, J.P. Segal1, C.W. Lees2, A. Hart1
1IBD Unit, St Mark’s Hospital Academic Institute, London, UK, 2Gastrointestinal Unit, Western General Hospital, Edinburgh, UK
Background
In 2016, the top 10 research priorities in treatment of inflammatory bowel diseases (IBD) were outlined by a group of clinicians, patients and patient-support organisations based in the UK, using the infrastructure of the James Lind Alliance (JLA) Priority Setting Partnership. Priority statements were ranked in order of perceived importance. The aim of this study was to measure the current distribution of these research priorities in European-led IBD clinical trials, ongoing or completed within the last 3 years, in light of the JLA recommendation. Pharmaceutical-led trials were excluded given the inherent bias towards drug conception and approval.
Methods
The database from Clinicaltrials.gov and European Union Clinical Trials Register were used to create an overview of non-pharmaceutical-driven European clinical studies involving adult patients with IBD. Trials posted on 09/08/2016 (publication date of the top 10 research questions) up to 16/11/2019 were included. The list was completed by trials found to be relevant, although not retrieved initially, based on author consensus.
Results
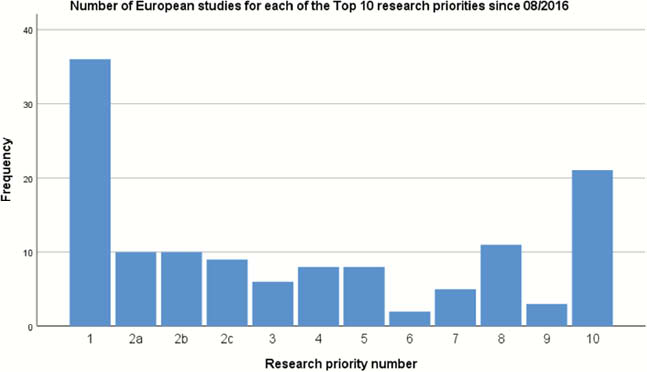
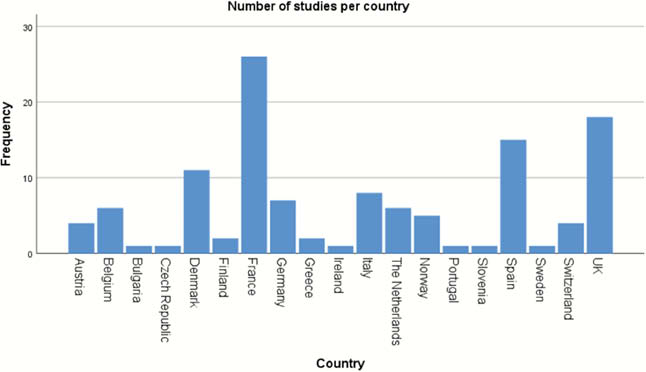
In total, 154 European non-pharmaceutical-funded clinical studies were found, of which 112 addressed one of the outlined top 10 IBD-research priorities and 8 addressed multiple topics simultaneously. Almost a third (30%) investigated the optimal treatment strategy considering efficacy, safety and cost-effectiveness (immunomodulators, biologics, surgery) in IBD (Priority 1). Development or assessment of biomarkers for stratification of patients (Priority 2) was the subject of 29 studies (24.2%). Twenty-one (17.5%) studies focused on altering gut microbiota (Priority 10). Eleven or fewer studies focused on fatigue, IBD-related pain and perianal Crohn’s disease (Priorities 4, 5 and 8). Priorities 3 and 7 concerning the role of diet in IBD management were evaluated in 9.2% studies. A minority of studies, 2.5% and 1.7%, respectively, addressed optimal timing for surgery in terminal ileal Crohn’s disease (Priority 9) and the best treatment for diarrhoea/incontinence (Priority 6). Of all 19 European countries, France, the UK and Spain accounted for almost half of all reviewed studies (49.2%).
Conclusion
Since publication of the top 10 research priorities in IBD treatment, non-pharmaceutical-funded research has mostly been focusing on development and validation of new therapeutic strategies, investigation of biomarkers and the role of gut microbiota. The latter topic has gained significant interest in IBD research, more so than higher-ranked Priority statements 3 to 9. Further research should prioritise the potential benefit of dietary interventions and patient-reported outcomes, such as management of IBD-related pain, fatigue and faecal incontinence.