
P601 Real World Evidence on the comparative effectiveness of Ustekinumab vs anti-TNF in Crohn’s disease with Propensity Score adjustment: maintenance phase results from the prospective observational RUN-CD study
Bokemeyer, B.(1);Plachta-Danielzik, S.(2);di Giuseppe, R.(2);Deppe, H.(3);Mohl, W.(4);Teich, N.(5);Hoffstadt, M.(6);Schweitzer, A.(7);von der Ohe, M.(8);Gauss, A.(9);Atrya, R.(10);Krause, T.(11);Blumenstein, I.(12);Höchstödter, J.(2);Hartmann, P.(3);Schreiber, S.(13);
(1)Interdisciplinary Crohn Colitis Centre Minden- Germany and Clinic of General Internal Medicine I- University Hospital Schleswig-Holstein- Campus Kiel- Germany, Gastroenterology, Minden, Germany;(2)Competence Network IBD, Kiel-Germany, Kiel, Germany;(3)Gastroenterology Practice Minden, Gastroenterology, Minden, Germany;(4)Gastroenterology Practice Saarbrücken- Germany, Gastroenterology, Saarbrücken, Germany;(5)Internistische Gemeinschaftspraxis für Verdauungs- und Stoffwechselkrankheiten Leipzig, Gastroenterology, Leipzig, Germany;(6)Gastroenterology Practice Isterlohn, Gastroenterology, Iserlohn, Germany;(7)Gastroenterology Practice Münster, Gastroenterology, Münster, Germany;(8)Gastroenterology Practice Herne, Gastroenterology, Herne, Germany;(9)University Clinics of Heidelberg-Heidelberg-Germany, Department of Gastroenterology- Internal Medicine IV, Heidelberg, Germany;(10)University Hospital Erlangen- University of Erlangen-Nürnberg Erlangen- Erlangen- Germany, Department of Medicine- Medical Clinic 1, Erlangen, Germany;(11)Gastroenterology Practice Kassel, Gastroenterology, Kassel, Germany;(12)Johann Wolfgang Goethe University Clinic- 60590 Frankfurt- Germany, Department of Gastroenterology and Clinical Nutrition, Frankfurt, Germany;(13)University Hospital Schleswig-Holstein- Campus Kiel- Germany, Clinic of General Internal Medicine I, Kiel, Germany;
Background
Observational real world studies are required in addition to RCTs which typically represent selected patients not reflecting everyday clinical practice. Between 2017-2020 patients with Crohn’s disease (CD) receiving a newly initiated biologics therapy were consecutively enrolled into the prospective, observational RUN-CD registry from 44 IBD-experienced German centres to assess effectiveness and safety of ustekinumab (UST) with a 3 years follow-up. Here, the results on the effectiveness of the maintenance therapy over 12 months are presented as a real world evidence (RWE) comparison of UST vs anti-TNF.
Methods
After exclusion of other biologics than UST and anti-TNF and missing outcomes, the final sample consisted of 607 CD-patients. Clinical remission (HBI ≤ 4) was the predefined endpoint at month 12. Patients were analyzed on a modified intent-to-treat basis (mITT; switchers considered as outcome failure). To reduce the effect of confounders, propensity score (PS) adjustment with inverse probability of treatment weighting (IPTW) was implemented. A weighted logistic regression was used, and the results were reported as odds ratio (OR) and 95% confidence interval (CI).
Results
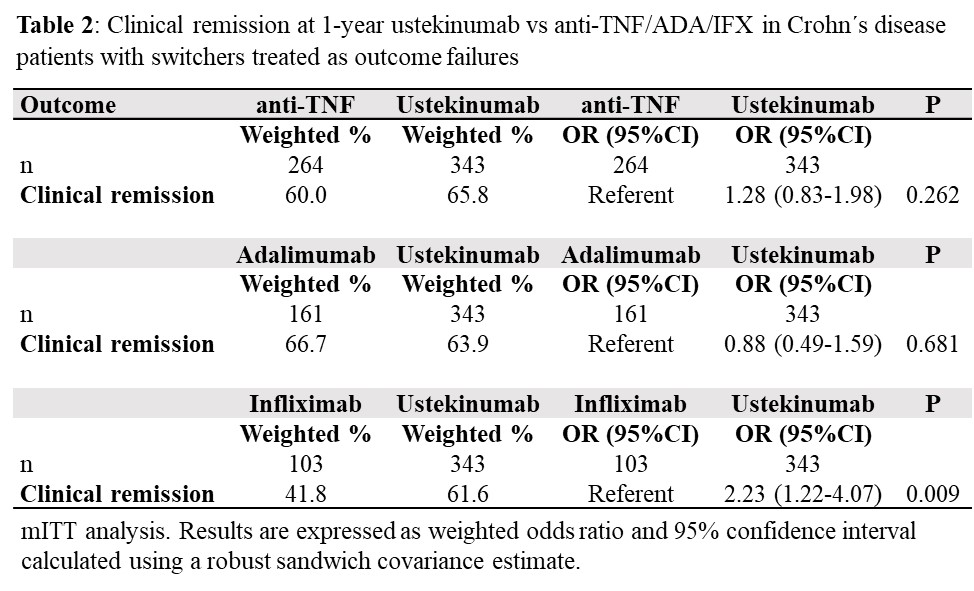
343 UST (naïve: 35) and 264 anti-TNF (naïve: 175) (ADA 61%, IFX 39%) CD-patients were included. PS removed systematic differences between both groups (mean of both groups: 15% perianal disease, 36% surgical resection, 41% EIM). Overall, the number of switches was lower in the UST group than in the anti-TNF group (Tab. 1). However, the number of switches within 12 months was significantly lower in the UST group only when compared to the IFX group (16.3% vs 27.2%; p=0.045) (Fig. 1). Clinical remission rates at 1 year (Tab. 2) were not statistically different for the overall UST vs. anti-TNF groups (65.8% vs 60.0%). Remission rates were similar for UST vs ADA, while these were significantly higher for UST vs. IFX (61.6% vs 41.8%; p=0.009). Looking at clinical remission in the week 16 responder group (Tab. 3), a statistically significantly higher remission rate was found in the overall group for UST (77.6%) vs anti-TNF (65.4%) (p=0.041), which was mainly driven by the higher UST remission rate in biologic-naïve CD patients (p=0.026).


Conclusion
This 1-year maintenance phase RWE-comparison with UST vs anti-TNF showed remarkably high clinical remission rates in both groups. Also due to a more frequent switching within the IFX group, the clinical remission rate at 1 year was significantly higher with UST than with IFX and higher with UST vs anti-TNF in the biologic-naïve groups. These results support together with the known favorable safety profile consideration of UST as a first-line targeted therapy for CD.