
P625 Kinetics and outcomes of transmural healing in patients with Crohn’s disease treated with anti-TNF therapy
C. Pastaud1, C. Hordonneau2, C. Lambert3, J. Vignette1, B. Pereira3, A. Buisson1
1CHU Estaing, Department of Digestive and Hepatobiliary Medicine- Department of Gastroenterology, Clermont-Ferrand, France, 2CHU Estaing, Radiology Department, Clermont-Ferrand, France, 3CHU, Biostatistics Unit, Clermont-Ferrand, France
Background
Transmural healing is a promising target in Crohns’ disease (CD) but remains poorly investigated. We aimed to evaluate the kinetics of transmural healing in CD treated with anti-TNF and to assess whether transmural healing is associated with more favourable outcomes.
Methods
It was a retrospective study from an MRI database of 449 patients performing MRI for luminal CD. Inclusion criteria were: CD patients older than 18 years-old receiving anti-TNF therapy, with an objective sign of inflammation on morphological evaluation (endoscopy or cross-sectional imaging), who underwent at least one MRI examination to assess therapeutic efficacy and follow-up longer than 6 months. Patients treated with anti-TNF agents for treat isolated perianal lesions were excluded. We used a statistical model based on imputation according to the last observation carry forward and clinical relevance. Each CD MRI lesions were then assessed every month during the first year. For segmental analysis, we used a division into six segments (jejunum, ileum, right colon, transverse colon, left/sigmoid colon and rectum). Transmural healing was defined as no MRI lesions.
Results
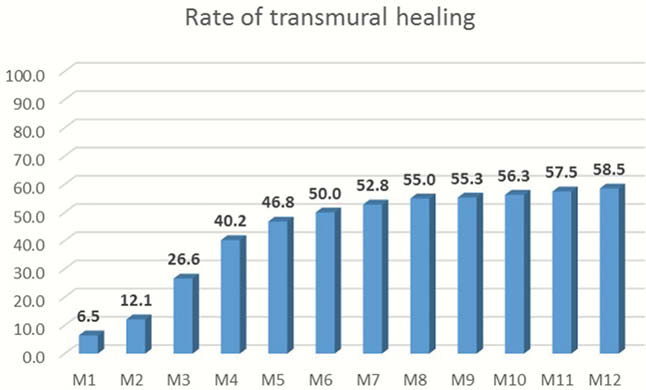
Overall, 148 patients were included. Among them, 81 were female (55.7%), 43 (34.4%) were current smokers and 56 (37.8%) had prior intestinal resection. The median CD duration at baseline was 7.6 years [1.4–15.2]. At baseline, 80 patients (54.4%) were anti-TNF-naïve. During the study, 69 patients (46.6%) were treated with infliximab, 77 patients (52%) received adalimumab while only 2 patients (1.4%) were treated with golimumab A combination therapy with thiopurines or methotrexate was found in 108 patients (74.0%) and 30 patients (20.3%) received concomitant steroids at the time of inclusion. Among 148 patients and 303 MRIs, 387 segments were analyzed. The rate of transmural healing was optimal between M6 and M8 and plateaued from the eighth month. The kinetics of transmural healing in CD patients treated with anti-TNF agents is presented in Figure 1.
Among the 148 patients with CD, 29 patients underwent intestinal resection (19.6%), 32 patients (21.6%) required an hospitalisation due to CD and 61 patients (41.2%) discontinued anti-TNF for therapeutic failure. In multivariable analyses, transmural healing was associated with decreased risk of surgery (HR=0.19[0.04–0.86];
Conclusion
Transmural healing, which is associated with better outcomes in CD, can be achieved in more than half of patients with CD. The best time to assess transmural healing was between 6 to 8 months after starting anti-TNF therapy.