
P650 Outcomes of endoscopic balloon dilation for luminal strictures in Crohn’s disease
R. Sarraj, M. Martinho, F. Bravo, E. Benz, P. Juillerat
Inselspital Bern, Gastroenterology- Clinical for Visceral Surgery and Medicine, Bern, Switzerland
Background
Luminal strictures are common complications of Crohn’s disease (CD). Endoscopic balloon dilation (EBD) is an alternative to surgery for CD strictures. (1–3). The aim of this study was to evaluate the EBD success rate and identify predictive factors in CD patients.
Methods
27 consecutive patients with CD in whom EBD was performed at the outpatient clinic of Bern University Hospital were retrospectively included in this study. Clinical, laboratory and endoscopic data were collected from the patient files. Stricture characteristics, short-term procedure success, procedure-related complications, occurrence of surgery and long-term clinical endpoints were documented. Short-term procedure success was defined by the ability to pass an 11.5-mm-wide endoscope through the stricture after dilatation and the absence of any documented complications during a 1-week follow-up.
Results
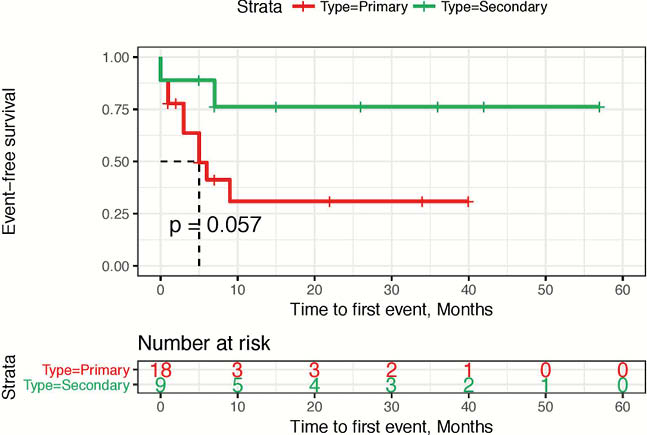
The study population consisted of 27 patients with Crohn’s disease. A total of 41 dilations were performed. 61.5% of the patients were on biologic therapy. The short-term dilatation success rate was 60%. 48.1% of the patients required stricture related surgery during the follow-up. There were two procedure-related complications 0.08% (bleeding; asymptomatic perforation discovered during surgery). 33.3% were anastomotic strictures. The median increase in dilatation diameter during a single session was 6 mm (range, 3–12mm). 53.8% of the patients required multiple dilatations during the same endoscopic procedure. In the Kaplan–Meier log-rank analysis, anastomotic strictures (secondary) did show a trend toward a longer surgery-free survival after EBD (
Conclusion
EBD is successful and safe in treating luminal strictures and in prevention of immediate surgery in a high proportion of CD patients, in particular for anastomotic stricture.
Cosnes J. Inflamm Bowel Dis 2002.
Rieder F. Gut 2013 / 3. Atreja A. J Crohns Colitis 2014.