
P658 Evolution of disease phenotype, time to biological therapy and medium-, long-term colectomy rates in Ulcerative Colitis patients in Western Hungary – a population-based study between 2007–2018, data from the Veszprem county cohort
Gonczi, L.(1);Lakatos, L.(2);Golovics, P.(3);Pandur, T.(4);David, G.(2);Erdelyi, Z.(2);Szita, I.(2);LakatosPhD, P.L.(1,5);
(1)Semmelweis University, Department of Medicine and Oncology, Budapest, Hungary;(2)Ferenc Csolnoky Hospital, Department of Gastroenterology, Veszprem, Hungary;(3)Hungarian Defence Forces- Medical Centre, Department of Gastroenterology, Budapest, Hungary;(4)Grof Esterhazy Hospital, Department of Gastroenterology, Papa, Hungary;(5)McGill University Health Centre, Department of Gastroenterology, Montreal, Canada;
Background
The number of prospective population-based studies evaluating the natural disease course and surgical outcomes of ulcerative colitis (UC) are still limited from Eastern Europe. The present study is a continuation of the Veszprem IBD population-based cohort with a follow-up of the incidence and disease course of IBD since 1977. Our aim was to evaluate disease course by examining progression in disease phenotype, time to biological therapy and colectomy rates in a prospective population-based database from Veszprem Province, including incident UC patients diagnosed between January 1, 2007 and December 31, 2018.
Methods
Data of 467 incident UC patients were analyzed (male/female: 236/1231; median age at diagnosis: 36 years(y) [IQR: 25-54]). Both in-hospital and outpatient records were collected and comprehensively reviewed at diagnosis and during clinical follow-up. The mean length of follow-up was 8.34y (SD: 3.5). Disease phenotype was evaluated based on the Montreal classification. Probability of medium-, long-term change in disease course and surgical outcomes were analyzed using Kaplan–Meier survival analysis.
Results
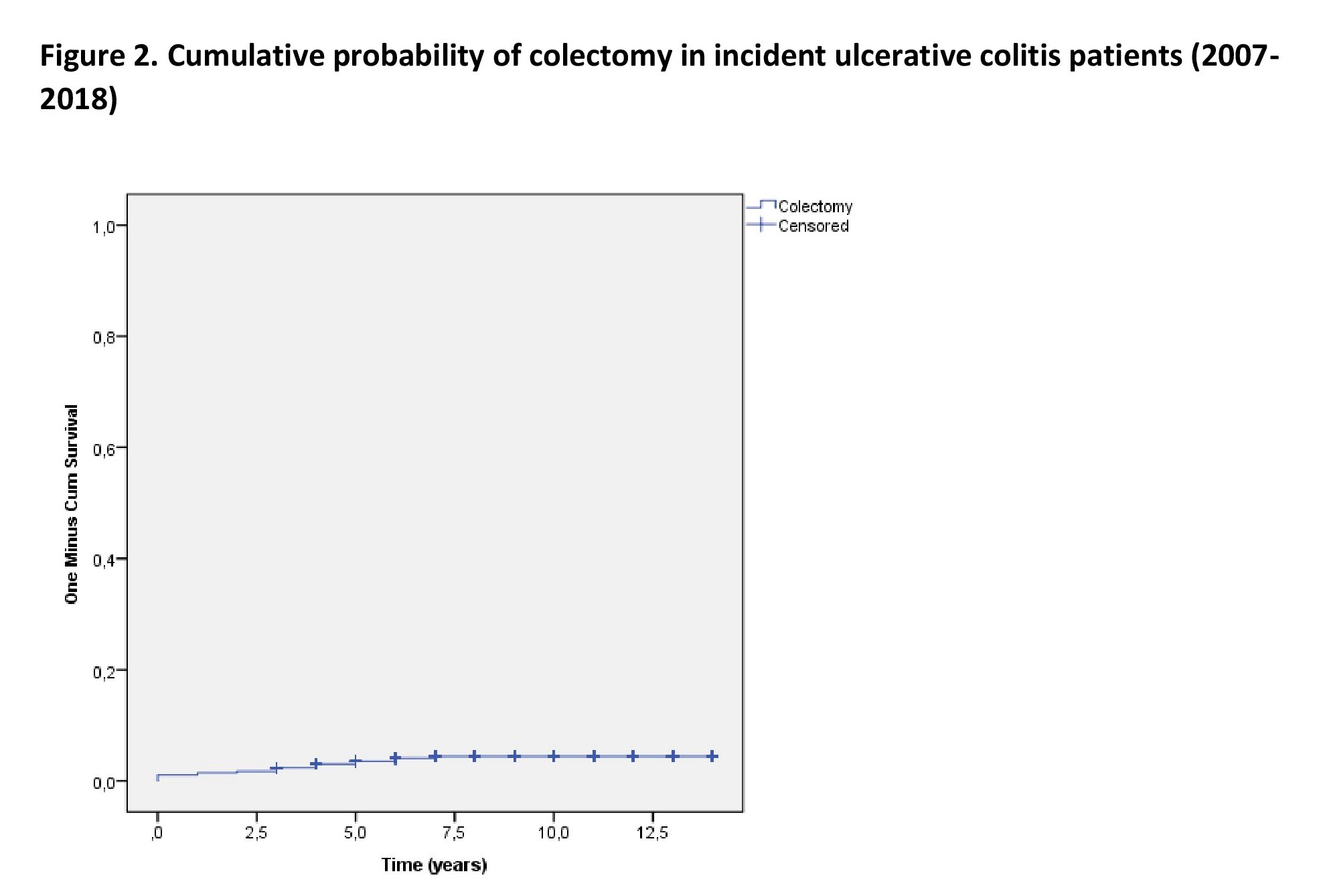
Disease extension was proctitis (E1), left sided colitis (E2), and extensive colitis (E3) in 22.3%/ 43.9%/ 33.8% of patients at diagnosis. The probability of disease progression into more extensive phenotype was 6.9% (SE:1.2) at 3 years, 8.3% (SE:1.3) at 5 years and 11.3% (SE:1.6) at 10 years. Figure 1. The Probability of receiving biological therapy after diagnosis was 9.9% (SE:1.4) at 3 years, 13.9% (SE:1.6) at 5 years and 17.8% (SE:2.0) at 10 years in this cohort. Overall colectomy rate was 4.1% in the total population at the end of follow-up. The probability of colectomy was 1.5% (SE:0.6) at 1 year, 3.6% (SE:0.9) at 5 years and 4.4% (SE:1.0) at 10 years in Kaplan-Meier analysis. Figure 2.

Conclusion
The probability of progression in disease extent was low overall, similar to results from recent pan-European population-based data. (Burisch 2019, JCC). Medium- and long-term colectomy rates were lower compared to Western European centers, but somewhat higher compared to our previous data from the Veszprem cohort (2002-2006). (Lakatos 2011, IBD).