
P724 Delaying an infliximab infusion by more than 3 days is associated with a significant reduction in trough levels
B. Ungar1,2, Z. Ben-Shatach1,2, T. Ziv-Baran2,3, E. Fudim1,2, M. Yavzori1,2, O. Picard1,2, L. Selinger1,2, B. Weiss2,4, U. Kopylov1,2, R. Eliakim1,2, S. Ben-Horin1,2
1Department of Gastroenterology, Sheba Medical Center- Tel Hashomer, Ramat gan, Israel, 2Tel-Aviv University, Sackler School of Medicine, Tel Aviv, Israel, 3Department of Epidemiology and Preventive Medicine, School of Public Health, Tel Aviv, Israel, 4Department of Pediatric Gastroenterology, Sheba Medical Center- Tel Hashomer, Ramat gan, Israel
Background
An association between higher infliximab-trough-levels (TL) and better outcomes has been demonstrated among IBD patients. Although standard scheduled infliximab therapy regimen consists of infusions at pre-defined time-points (weeks 0, 2, 6 and every 8 weeks), short-period deviations from therapeutic schedule are common in ‘real life’, especially during maintenance period (due to weekends, holidays, concurrent illnesses, etc.). We aimed to determine whether short-period deviations from infusion-schedule affect infliximab-TL and therapy outcome.
Methods
This was a retrospective study, analysing sera from all IBD patients receiving infliximab maintenance-therapy every 8 weeks in a tertiary medical centre. Associations between time since last infusion and TL were analysed. Clinical scores were recorded prospectively on infusion days and baseline demographic parameters were derived from patients’ charts. Statistical analysis was performed using generalised estimating equations.
Results
In total, 2088 sera of 302 maintenance-period infliximab-therapy-patients were included (median TL 4.1 μg/ml, IQR 2.3–6.5 μg/ml). A delay beyond 3 days in infusion (
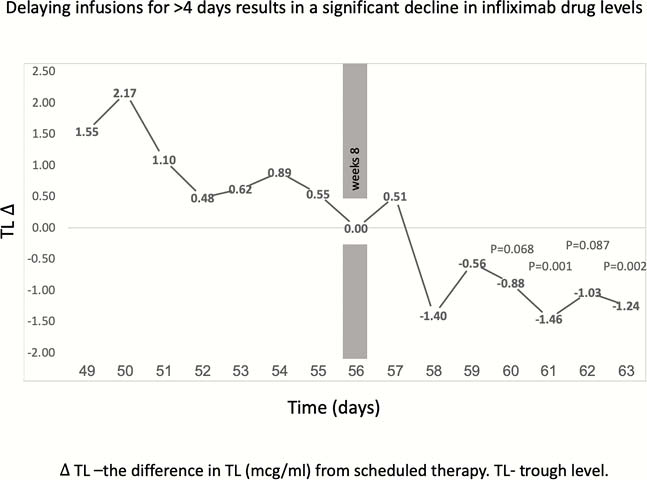
Conclusion
Real life delays of <4 days from infusion protocol can probably be allowed. Delays beyond that would significantly decrease TL and might negatively affect therapy outcome. As patients arriving late for an infusion had higher rates of clinical remission than those arriving early, we assume clinical factors mainly drive patients to receive an earlier-then-scheduled infusion.